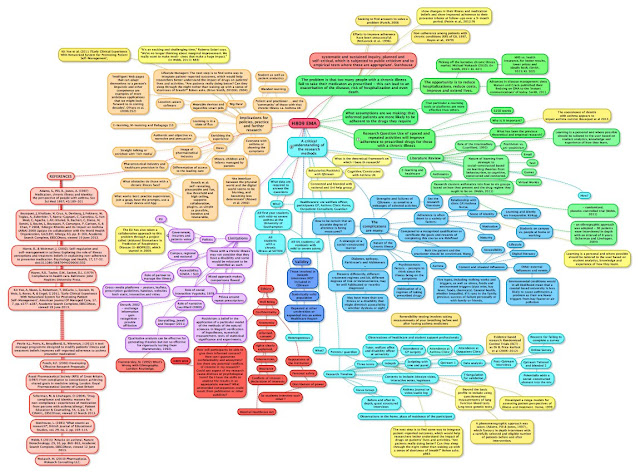
Fig.1 H809 EMA Mindmap (for fellow H809 / MA ODErs I've added a PDF version in the TMA Forum) Created using Simpleminds.
- H809 - Practice-based research in e-learning
- MA ODE - Masters in Open and Distance Education
- TMA - Tutor Marked Assignment
- PDF - PDF
Yonks ago I realised for me the best time to study was v.early in the morning. 4.00 am to breakfast isn't unusual, 5.00 am is more typical. All it costs is an early night. This is easy too - no television. Its move from the shed to the dump is imminent.
A week ahead of schedule I find I have an EMA to complete - this'll give me a three hour, exam like run of it. Even the dog knows not to bother me.
For those on the same path the mindmap of my H809 EMA is above.
Ask if you're interested in a legible PDF version.
This gorse bush off density has patterns within it that I can decipher. The net result ought to come out somewhere around the 4,000 word mark too. This approach could not be more different to my earliest TMAs and EMAs three years ago - they were too often the product of what I call 'jazz writing' (this kind of thing), just tapping away to see where it takes you. This process used to start on scrolls of backing wallpaper taped to my bedroom wall. Now it goes onto a whiteboard first.
As always this blog is an e-portfolio: most notes, moments in student forums and references are in here.
I recommend using a blog platform in this way. You can default to 'private', or share with the OU community ... or 'anyone in the world'. One simple addition to this would be a 'share with your module cohort'.
By now I have clicked through some 165 posts taggeed H809 and can refer to H809ema for those picked out for it.
One split occured - I very much wanted to explore the use of augmented reality in museum visits, but found instead a combination of necessity and logic taking me back to the H809 TMA 01 and a substantial reversioning of it. Quite coincidentally this proposed research on adherence to preventer drugs amongst moderate to severe asthmatics had me taking a very close interest on a rare visit to a hospital outpatient's. Nasal endoscopy must look like a circus trick to the casual observer as the consultant carefully 'lances' my skull through the nose with a slender and flexible rod on which there is a tiny camera and light. 'Yes, I can see the damage from surgery' he declares (this was 33 years ago), 'but no signs of cancer'.
There's a relief.
An unexplained nose bleed lasting the best part of 10 weeks was put down to my good-boy adherence to a steroid nasal spray that had damaged the soft tissue. And the medical profession wonder why drug adherence can be so low? 20% to 60% 33 years on and courtesy of the OU Library I found a wholly convincing diagnosis - allergic rhinitis. The 'paper' runs to over 80 pages excluding references and has some 20 contributors (Bousquet, 2008). I'll so miss access to the online library as most papers appear to cost around the £9 to download. This desire to remain attached by a digital umbilical chord to such a resource is one reason I wish to pursue yet more postgraduate studying and potentially even an academic career. I get extraordinary satisfaction browsing 'stuff' to feed my curiosity.
When I stop diddling around here I'll pick off this mindmap in a strick clockwise direction from around 1 O'Clock.
Simpleminds is great as a free App. It's taken me a couple of years to get round to paying £6 for a version that can be exported into a word file though I rather enjoy the slower, more considered 'cut and paste' which adds another opportunity to reflect, expand or ditch an idea.
REFERENCE
Bousquet, J, Khaltaev, N, Cruz, A, Denburg, J, Fokkens, W, Togias, A, Zuberbier, T, Baena-Cagnani, C, Canonica, G, Van Weel, C, Agache, I, Aït-Khaled, N, Bachert, C, Blaiss, M, Bonini, S, Boulet, L, Bousquet, P, Camargos, P, Carlsen, K, & Chen, Y (2008) 'Allergic Rhinitis and its Impact on Asthma (ARIA) 2008 Update (in collaboration with the World Health Organization, GA2LEN', Allergy, 63, pp. 8-160, Academic Search Complete, EBSCOhost, viewed 19 June 2013.